
Full-field digital mammography (FFDM) offers many advantages over film/screen mammography. Although most commercial FFDM systems have shown to have superior image quality over their analog counterparts – as measured through detective quantum efficiency (DQE) – large scale clinical trials have failed to demonstrate the expected improved diagnostic efficiency. The main reason for the diagnostic’s impairment of conventional mammography (both film/screen and FFDM) is the fact that the 3-D anatomical information is projected into a 2-D image plane. Therefore, anatomical structures that overlap the tumors – and not inherent signal-to-noise ratio of the image – limit the radiologist’s ability to detect certain cancers. Digital tomosynthesis for mammography has shown promise to overcome this limitation of conventional mammography by acquiring several views of the breast from different angles and reconstructing the image into a 3-D volume set.
In 1972, Grant described a type of geometric tomography called tomosynthesis, which uses a conventional x-ray source and a digital detector to produce a virtually unlimited number of tomographic images at arbitrary depths in the patient. Tomosynthesis has recently enjoyed a resurgence due to several key technological developments including flat-panel detectors capable of producing high-speed, high-quality digital images, as well as reconstruction and post-processing algorithms which reduce the blur from out-of-plane structures, thereby rendering section images of much higher quality. Successful reconstruction and post-processing algorithms have included filtered back projection and traditional shift-and- add reconstruction coupled with matrix inversion or constrained iterative restoration deblurring methods.
Breast tomosynthesis promises to improve the detection and characterization of lesions by removing overlapping dense fibro glandular tissue. The goal is to provide 3-D information at high resolution and comparable dose to mammography.
A prototype breast tomosynthesis system will be presented based on a modified full-field digital mammography device and an amorphous silicon detector suited for fast readout. The goal of this prototype tomosynthesis system is to serve as a R&D tool to gain experimental insight into the tradeoffs between acquisition speeds, reconstruction algorithms, number of views, angular span for x-ray tube, x-ray spectrum, and many other parameters which affect tomosynthesis image quality, and patient glandular dose.
A X-ray generator was modified to allow for an x-ray tube motion to cover an arc of ±25° relative to the pivoting point that is 6 cm above the detector surface. Hardware and software modifications were also made to the machine to allow multiple x-ray pulses to be generated during a single x-ray exposure sequence, and synchronize the x- ray pulses with the detector read/integrate cycle and x-ray tube motion. In order to get rid of mechanical instabilities as much as possible, a mode with continuous tube motion was selected instead of a “step and shoot” mode which might induce vibrations. The integrated tomosynthesis system is shown in Figure 1.
-600x400.png) Figure 1: Photograph of prototype tomosynthesis system.
Figure 1: Photograph of prototype tomosynthesis system.
The detector used in this prototype tomosynthesis system is a direct converter amorphous selenium flat-panel detector. The pixel matrix are 3,108 × 3,956 , with a pixel pitch of 77 µm, which translates to an active area of 10 inch × 12 inch. The electronic gain and read time of the detector were optimized for tomosynthesis imaging. A photograph of the x-ray detector is shown in Figure 2.
Figure 2: Photograph of CsI Full Field Digital Wired Mammography Diagnostic X-ray Imaging Flat Panel Detector (MMD1012, e-Join, China).
Human subjects were recruited from among cases already scheduled to undergo biopsy. One of the scans acquired at Duke Medical Center is shown in Figure 3. The human subject with compressed breast thickness of 6 cm underwent tomosynthesis scans on each breast in MLO position. The anode/filter combination was W/Rh with 28kVp. According to the experimental exposure tables for the FFDM system with the same tube, 133.4 mAs were applied in total for 49 projections. Figure 3 (left) displays a slice through the middle section of the compressed breast, where clearly the ducts and other fine structure are visible. Most prominent is a new invasive ductal carcinoma with some lobular component in this patient who had a biopsy 25 years ago16. In Figure 3 (right) a slice close to the upper surface of the breast is shown depicting the blood vessels.
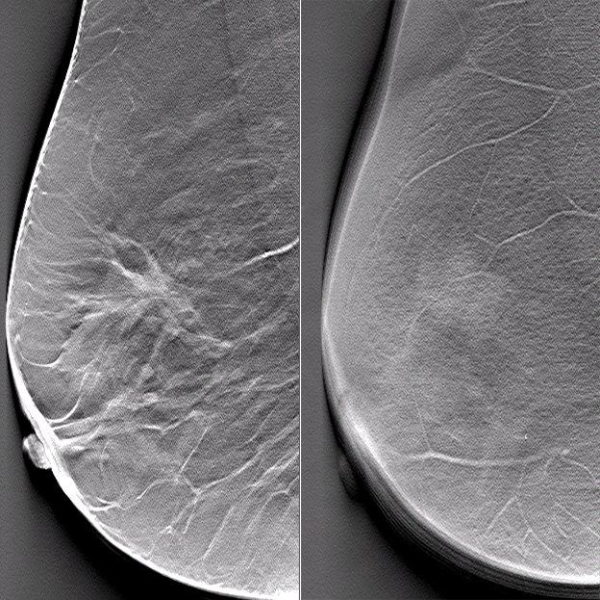
Figure 3: Reconstructed slices of a patient data set in MLO projections, (left) slice at z = 21 mm above patient table, (right) slice close to the surface of the breast.
We developed a research system for breast tomosynthesis based on an amorphous silicon direct detector with fast readout and low lag. The detector is designed for high DQE to enable operation at very low exposures. This low-noise feature of the detector is particularly important if one wants to split the total exposure to many single projections for tomosynthesis reconstruction. The tungsten x-ray spectrum provided by the system helps further reducing the dose of a tomosynthesis scan.
-600x400.jpg)
We demonstrated the improvement of image quality by employing more projections than previously used for breast tomosynthesis. With a number of projections of 25 and more, the streak-like limited-number-of-view artifacts can be largely reduced. First patient images promise the high potential of this breast tomosynthesis system.